whole grain oats are naturally gluten-free, gut-friendly and heart-healthy!

Food Allergy Facts
Provided by www.foodallergy.org
Only Oats provides allergy FREE baked goods that cover most allergy categories
All of our Only Oats Cookies are:
non-dairy,
gluten-free
tree-nut and peanut-free
We also produce vegan cookies. All ingredients are clearly labeled on our website. We go to great lengths to insure that there is no cross-contamination in our products.
This makes Only Oats Cookies a smart choice for those with food allergies or intolerances. Browse our product pages according to the category which most interests you and addresses your dietary needs.
The information on this page was provided by www.foodallergy.org.
What is a Food Allergy?
A food allergy is “an adverse health effect resulting from a specific immune response that occurs reproducibly on exposure to a given food.”1
In plain language, a food allergy is when a person’s immune system overreacts to something in a certain food. This part of the food that the body reacts to is usually a protein and is called an allergen. The immune system thinks the allergen is a threat and tries to attack it. This response can cause a range of symptoms, which are called an allergic reaction.
To Which Foods are People Allergic?
More than 170 foods have been reported to cause food allergy reactions in the U.S.1
In 2004, eight major food allergens—milk, egg, peanuts, tree nuts, wheat, soy, fish and crustacean shellfish—were identified as responsible for at least 90 percent of the serious food allergy reactions in the U.S.1
In 2021, the U.S. added sesame as the ninth major food allergen.7
The most common food allergies in children are allergies to peanuts, milk, shellfish, and tree nuts.9
The most common food allergies in adults are allergies to shellfish, milk, peanuts, and tree nuts.7
How Many People Have Food Allergies?
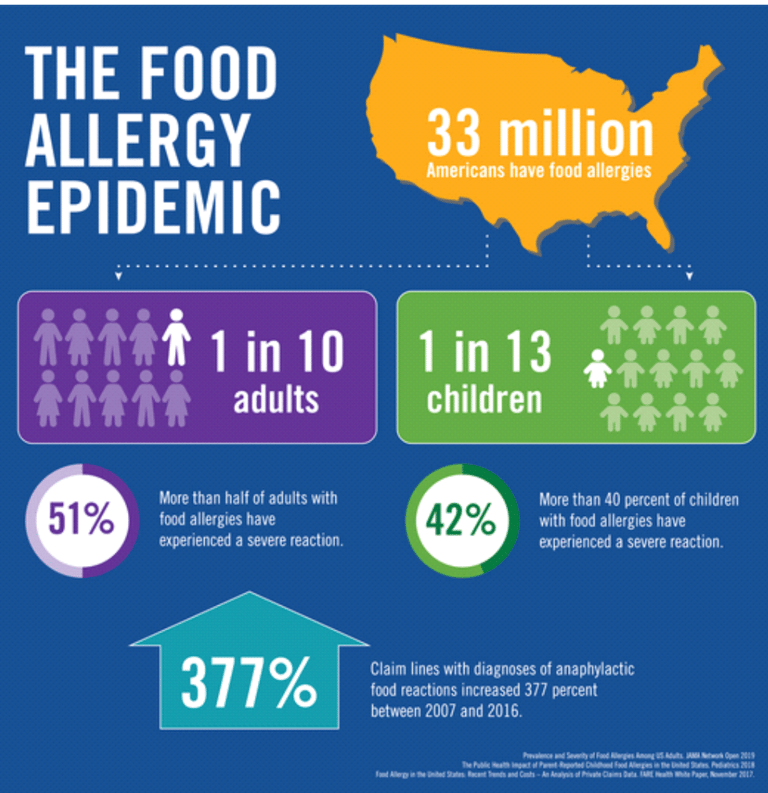
Approximately 33 million people in the United States have at least one food allergy.7,8,9
Nearly 11 percent of adults aged 18 or older have at least one food allergy. This is more than 27 million adults.7,8
Results from a 2015–2016 survey of more than 38,000 children indicate that 5.6 million children, or nearly 8 percent of children, have food allergies.8,9 That’s one in 13 children, or roughly two in every classroom.
Studies published in 2018 and 2019 can be used to estimate the current number of U.S. children and adults who are allergic to specific foods.2,7,8,9
shellfish: 8.4 million
milk: 6.2 million
peanut: 6.2 million
tree nuts: 3.9 million
egg: 2.7 million
fin fish: 2.7 million
wheat: 2.4 million
soy: 1.9 million
sesame: 0.7 million
Based on a 2015–2016 survey an estimated 4.7 percent of U.S. children have a physician-diagnosed food allergy. However, a follow-up analysis of health care claims data found that among children insured through Medicaid, only 0.6 percent have a documented food allergy diagnosis, raising concerns about equitable awareness of and access to food allergy specialists.8
According to a 2021 National Health Interview Survey (NHIS) conducted by the National Center for Health Statistics (NCHS), a division of the Centers for Disease Control and Prevention (CDC), 5.8% of children aged 0–17 are diagnosed with a food allergy.10
About 40 percent of children with food allergies have multiple food allergies (more than one food to which they’re allergic).9
Serious Allergic Reactions (Anaphylaxis) Require Immediate Treatment
· An allergic reaction to food can have many symptoms. You can have different symptoms from one reaction to the next. Some may start with skin symptoms, like a rash. Serious symptoms, like a drop in blood pressure or trouble breathing, can put your life in danger.
· Rapid treatment with epinephrine (adrenaline) within minutes of the onset of anaphylaxis symptoms is necessary and crucial to successfully treating an anaphylactic reaction. A self-injectable epinephrine device is available by prescription.17
· Not recognizing the presence or severity of an anaphylactic reaction and/or a delay in treatment with epinephrine (i.e., greater than a few minutes) are risk factors for fatalities.18,19,20
· More than one dose of epinephrine may be required to effectively treat a severe food allergy reaction.17
· It is possible to have anaphylaxis without any skin symptoms, such as rash or hives.22
· Symptoms of anaphylaxis may recur a few hours after initially subsiding (known as a biphasic reaction). Experts recommend an observation period of 4 to 6 hours to monitor that the reaction has fully resolved.21,23
Food Allergies Impact Quality of Life
About one in three children with food allergies reports being bullied due to the food allergy. Moreover, among children with allergies to more than two foods, over half report being bullied due to food allergy.24
Compared to children who do not have a medical condition, children with food allergy are twice as likely to be bullied.25
More than one-quarter of parents surveyed during food allergy appointments report that their children do not participate in camp or sleepovers because of food allergy. More than 15 percent of the parents participating in this survey do not go to restaurants, and more than 10 percent avoid child care settings or playdates at friends’ houses. Ten percent of the parents home-school their children to prevent food allergen exposure.26
In another report, among parents of young children in the first year after food allergy diagnosis, most avoid restaurants and about half restrict social activities or travel.25
Mothers of food-allergic children under age five have significantly higher blood-pressure measurements and report significantly greater levels of psychosocial stress than mothers whose preschool-aged children do not have food allergies.27
Works Cited
NIAID-Sponsored Expert Panel. Guidelines for the diagnosis and management of food allergy in the United States: Report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010; 126(6):S1-58.
Warren CM, Chadha AS, Sicherer SH, Jiang J, Gupta RS. Prevalence and Severity of Sesame Allergy in the United States. JAMA Network Open 2019; 2(8):e199144. DOI: 10.1001/jamanetworkopen.2019.9144.
Davidson L, Jones B. The Racial and Ethnic Makeup of Food Allergy Immunotherapy Trials. J Allergy Clin Immunol. 2021 147(2), Feb. 1, 2021 Supplement, Abstract 93.
Mahdavinia M, Fox SR, Smith BM, James C, Palmisano EL, Mohammed A, Zahid Z, Assa’ad AH, Tobin MC, Gupta RS. Racial Differences in Food Allergy Phenotype and Health Care Utilization Among US Children. J Allergy Clin Immunol Pract. Mar-Apr 2017;5(2):352-357.e1.
Warren C, Lei D, Sicherer S, Schleimer R, Gupta R. Prevalence and characteristics of peanut allergy in US adults. J Allergy Clin Immunol. June 2021; 147(6): 2263-2270.E5.
U.S. Food and Drug Administration. Food Allergen Labeling and Consumer Protection Act of 2004 (FALCPA). Updated March 7, 2022. https://www.fda.gov/food/food-allergensgluten-free-guidance-documents-regulatory-information/food-allergen-labeling-and-consumer-protection-act-2004-falcpa. Accessed May 20, 2022.
Gupta RS, Warren CM, Smith BM, Jiang J, Blumenstock JA, Davis MM, Schleimer RP, Nadeau KC. Prevalence and Severity of Food Allergies Among US Adults. JAMA Network Open 2019; 2(1):e185630.doi:10.1001/jamanetworkopen.2018.5630.
U.S. Census Bureau. Age and Sex Composition in the United States: 2022. Retrieved from https://www.census.gov/data/tables/2022/demo/age-and-sex/2022-age-sex-composition.html on September 7, 2023.
Gupta RS, Warren CM, Smith BM, Blumenstock JA, Jiang J, Davis MM, Nadeau KC. The Public Health Impact of Parent-Reported Childhood Food Allergies in the United States. Pediatrics 2018; 142(6):e20181235.
Zablotsky B, Black LI, Akinbami LJ. Diagnosed allergic conditions in children aged 0–17 years: United States, 2021. NCHS Data Brief, no 459. Hyattsville, MD: National Center for Health Statistics. 2023. DOI: https://dx.doi.org/10.15620/cdc:123250.
Jackson KD, Howie LD, Akinbami LJ. Trends in allergic conditions among children: United States, 1997-2011. NCHS data brief, no 121. Hyattsville, MD: National Center for Health Statistics. 2013. Retrieved from http://www.cdc.gov/nchs/products/databriefs/db121.htm.
Sicherer SH, Muñoz-Furlong A, Godbold JH, Sampson HA. US prevalence of self-reported peanut, tree nut, and sesame allergy: 11-year follow-up. J Allergy Clin Immunol. 2010; 125(6):1322-1326.
Keet CA, Savage JH, Seopaul S, Peng RD, Wood RA, Matsui EC. Temporal trends and racial/ethnic disparity in self-reported pediatric food allergy in the United States. Ann Allergy Asthma Immunol. 2014 Mar; 112(3):222-229.
U.S. Department of Education, Office for Civil Rights. Questions and Answers on the ADA Amendments Act of 2008 for Students with Disabilities Attending Public Elementary and Secondary Schools. https://www2.ed.gov/about/offices/list/ocr/docs/dcl-504faq-201109.html. Accessed May 20, 2022.
Gupta R, Holdford D, Bilaver L, Dyer A, Holl JL, Meltzer D. The economic impact of childhood food allergy in the United States. JAMA Pediatr. 2013 Nov; 167(11):1026-31.
Bilaver LA, Kanaley MK, Fierstein JL, Gupta RS. Prevalence and Correlates of Food Allergy Among Medicaid-Enrolled United States Children. Acad Pediatr. Jan-Feb 2021;21(1):84-92.
American Academy of Allergy, Asthma and Immunology, and American College of Allergy, Asthma and Immunology. Joint Task Force on Practice Parameters; Joint Council of Allergy, Asthma and Immunology. The diagnosis and management of anaphylaxis: an updated practice parameter. J Allergy Clin Immunol. 2005; 115:S483-523.
Bock SA, Muñoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001–2006. J Allergy Clin Immunol. 2007; 119(4):1016-1018.
Bock SA, Muñoz-Furlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J Allergy Clin Immunol. 2001; 107(1):191-193.
Sampson HA, Mendelson L, Rosen J. Fatal and near-fatal anaphylactic reactions to food in children and adolescents. N Engl J Med.1992; 327(6):380-384.
Korenblat P, Lundie MJ, Danker RE, Day JH. A retrospective study of epinephrine administration for anaphylaxis: how many doses are needed? Allergy Asthma Proc. 1999; 20:383-386.
Sampson HA. Anaphylaxis and Emergency Treatment. Pediatrics 2003; 111(S6):1601 -1608.
Ellis AK, Day JH. Incidence and characteristics of biphasic anaphylaxis: a prospective evaluation of 103 patients. Ann Allergy Asthma Immunol. 2007 Jan; 98(1) 64-69.
Shemesh E, Annunziato RA, Ambrose MA, Ravid NL, Mullarkey C, Rubes M, Chuang K, Sicherer M, Sicherer S. Child and parental reports of bullying in a consecutive sample of children with food allergy. Pediatrics 2013; 131:e10-e17.
Herbert L, Shemesh E, Bender B. Clinical management of psychosocial concerns related to food allergy. J Allergy Clin Immunol Pract. 2016; 4(2):205-213.
Bollinger ME; Dahlquist LM, Mudd K; Sonntag C, Dillinger L, McKenna K. The impact of food allergy on the daily activities of children and their families. Ann Allergy Asthma Immunol. 2006; 96:415-421.
Walker SO, Mao G, Caruso D, Hong X, Pongracic JA, Wang X. Cardiovascular risk factors in parents of food-allergic children. Medicine (Baltimore). 2016 Apr; 95(15): e3156.
Delicious
Gluten-free cookies, cakes, bread and muffins made from whole oats and grain free sesame cookies
Nutritious
Heart-healthy
26@onlyoatscookies.com
1-917-600-9632
© 2025. All rights reserved.